Facilitated Opioid Workshops in Tennessee
Like many other states, Tennessee is facing an opioid epidemic. In 2016, 1,186 people died of an opioid overdose in the state. That’s up from 698 opioid overdose deaths just four years prior.
As part of their Prevention for States activities, the Tennessee Department of Health chose to host three community summits and engaged the American Institutes for Research (AIR) to serve as a facilitator for these workshops in Nashville, Knoxville, and Memphis in April 2018. Stakeholders gathered at each workshop to share ideas; examine local opioid misuse, overdose and mortality data; and identify evidence-based promising strategies to strengthen their existing responses to the epidemic. More than 700 members of the community participated, representing local health, law enforcement, criminal justice, substance abuse and mental health, treatment, and the faith-based communities. Community members who are in recovery also attended.
“We adopted this approach to flip the script,” Dr. Melissa McPheeters, director of Informatics and Analytics, Department of Health, said. She added, “Rather than hosting a summit of ‘scientific experts,’ we wanted to showcase the communities as the experts in their own epidemic and learn from them how they interpreted data about their communities. We asked them to share efforts that were working or that they wanted to implement, and we invited them to interpret local data with support and guidance to think about new potential activities. Most importantly, we provided a venue for the real experts to make connections and commit to collaborations.”
AIR’s Work with Tennessee
Tennessee has explicitly chosen to focus on a data-driven response to the epidemic, and a good portion of this work is being led by the Office of Informatics and Analytics within the state Department of Health. That office focuses on developing advanced data-driven analysis and informatics and ensures that data are made available in accessible, clear formats (for example, using data visualizations). Certainly, however, data alone will not slow the epidemic; rather data can drive the choice of good and appropriate interventions at the community level. People on the front lines, in the communities, are best placed to know the real meaning behind the data–and which interventions are likely to make a difference at the local level. It’s these front-line individuals who need to be empowered with data to inform and guide their daily work in combating the epidemic.
AIR used its Community Data Interpretation (CDI) method to facilitate the second day of each workshop. The CDI process enables community members to gain a better understanding of their own data and fosters dialogue among policy makers and practitioners, from a range of systems, to design more effective solutions. At each table, AIR and the state’s Department of Health placed individuals from law enforcement, substance abuse and mental health, treatment, and faith-based communities, to jumpstart “cross-systems” conversations. In fact, this networking benefit was a widely cited boon of the CDI format among participants.
At each workshop, CDI consisted of five steps, engaging participants to:
- Understand and interpret data. Participants reviewed data visualizations of trends in opioid overdose deaths, inpatient and outpatient hospital visits, and prescription rates to get a clearer picture of what is happening in their areas. Participants also used Geographic Information System (GIS) maps to view state and regional data (see figure below for an example).
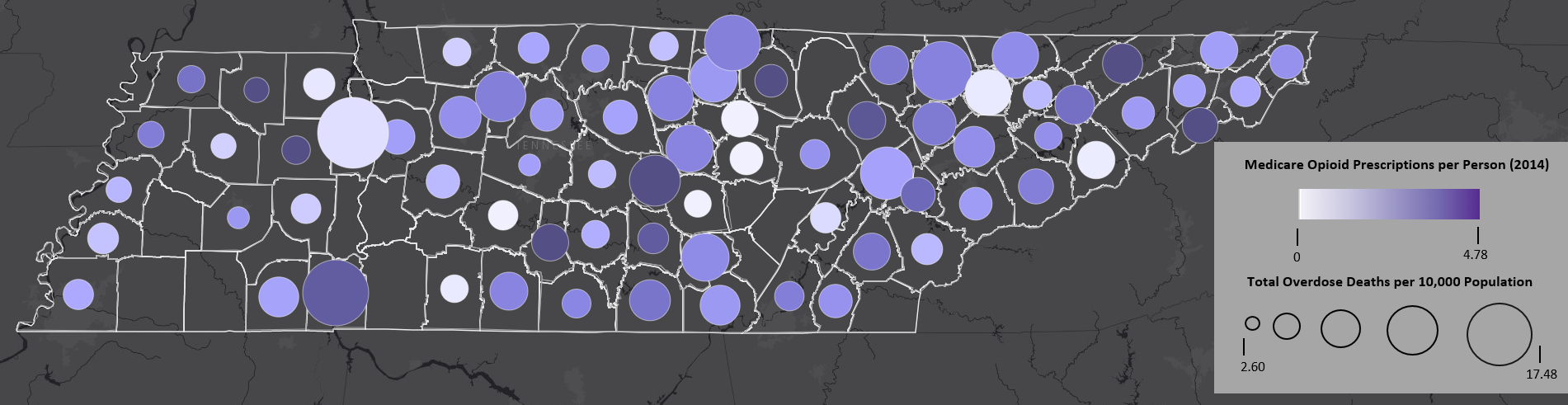
This map shows the relationship between the number of Medicare opioid prescriptions per person (2014) and the total overdose death rate in a county (2017). The size of the circles indicates the number of opioid prescriptions (with larger sizes indicating more prescriptions) per capita and the color of the circles indicates the per capita overdose death rate (with darker circles indicating more deaths). Sources: Data on the number of overdose deaths come from the County Health Rankings, produced by the Robert Wood Johnson Foundation from various national and state data sources. Data on Medicare opioid prescriptions come from the Centers for Medicare and Medicaid Services’ publicly available data.
- Identify and set priorities. Participants worked to answer: “Which factors contribute to our local opioid crisis? Which factors can we change and act upon most easily?”
- Explore evidence-based, promising interventions. With an emphasis on choosing practices that respond to data, and best fit a community’s needs, participants learned about a variety of approaches. For example, evidence-based solutions to reduce deaths include physician co-prescribing of naloxone with an opioid to patients identified as high-risk for opioid misuse and overdose. Additionally, participants learned about promising interventions in prevention, treatment, and law enforcement.
- Understand opportunities and challenges. Participants identified gaps in potential approaches, such as untapped and unused resources and where they might need additional help.
- Share knowledge and action items. Participants then shared ideas for next steps and lessons learned with the larger workshop groups and the Department of Health. For example, some groups discussed the lack of treatment options for many individuals living in remote rural areas. Participants then identified online treatment options to increase accessibility as a potential solution. In this type of program, patients with internet access receive individual counseling sessions through web-based videoconferencing, as well as medication-assisted treatment (MAT). Recently the Centers for Medicare and Medicaid Services (CMS) released Federal policy guidance to State Medicaid Directors along these lines.
Jennifer Loeffler-Cobia, senior researcher for AIR and project director for this work, remarked, “It was amazing to see stakeholders engage in collaborative conversations around data, and consider innovative responses they could implement together to reduce deaths and have an impact on this still growing problem. I hope to see more states take part in this type of data-driven approach.”
For more information
AIR has developed a suite of protocols and tools to engage policymakers and practitioners across systems in re-examining the data about how and where the opioid epidemic affects people in their state and communities. The process engages participants to improve planning processes based on data; weigh evidence-based interventions to achieve better, localized outcomes; consider implementation readiness; and enhance capacity to respond. For more information, please visit AIR’s Center for Addiction Research and Effective Solutions (AIR CARES).
This piece was written by Cheryl Vince, AIR Senior Vice President and Fellow, in partnership with Dr. Melissa McPheeters, Director of Information and Analytics, Tennessee Department of Health.
